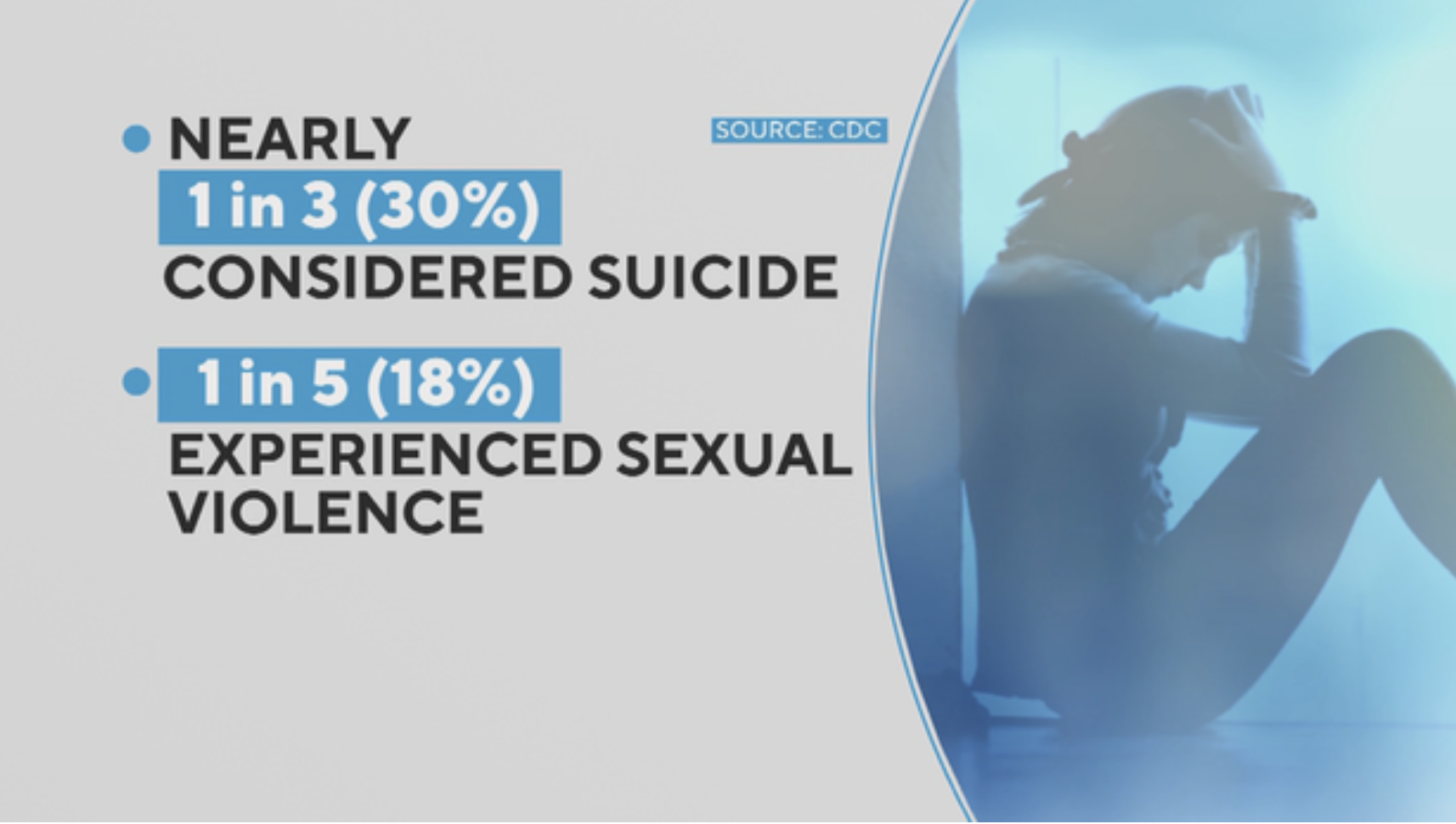
Courtesy CBS rendering of two CDC spring of 2021 survey findings about American high school girls reported Monday, Feb 13, 2022
by James C. Sherlock
The Centers for Disease Control and Prevention (CDC) is in full self-defense mode.
CDC and the left backed, indeed insisted, upon social isolation during the pandemic.
Now they deflect and deny agency in the consequences. They continue to try to insulate themselves from the catastrophic educational and mental health effects on children and adolescents of that social isolation.
A weakened CDC Director is pledging to overhaul the agency and its culture, a backhanded admission of the unimaginably bad performance of CDC during COVID.
The entrenched bureaucracy that is that agency and its culture is admitting nothing. They are counting the days until she leaves.
So, if experience counts for anything, we pretty much know how the CDC “overhaul” will work out.
Virginia is due for the same sort of review of state actions during COVID.
The Northam administration stumbled badly at nearly every new turn after failing to either exercise or implement Virginia’s own pandemic emergency plan. Which was excellent and predicted nearly exactly the course of events.
Then they tried to cover up the existence of that plan itself.
I am not sure that such a review is forthcoming. If it is, it will be preemptively be declared political. It must be done anyway.
The federal government, under progressive management, is “moving on.”
Or trying to.
I hope Virginia government does not make the same mistake. Continue reading