
Click for larger image
by James A. Bacon
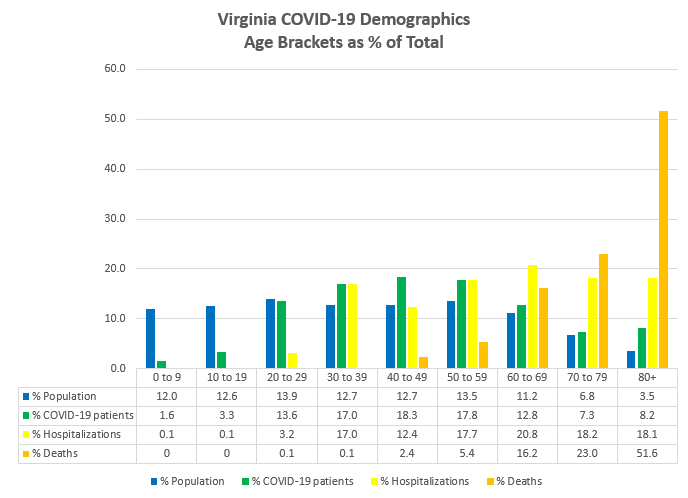
The COVID-19 virus, we have been told repeatedly strikes all ages. That statement is true, but also misleading. If one crunches the numbers from the Virginia Department of Health COVID-19 dashboard, there is no avoiding the conclusion that COVID-19 is a serious disease primarily for the middle-aged and elderly, and it kills mainly the elderly.
In the chart above, the blue bar breaks down each age bracket by the percentage it comprises of Virginia’s 8.5 million inhabitants. The green bar breaks down the percentage of confirmed COVID-19 patients in each age bracket. The yellow bar shows the percentage of hospitalizations in each bracket, and the orange bar the percentage of deaths.
A tiny percentage of Virginians under 20 years old have tested positive for COVID-19. If they do get it, their symptoms are rarely serious, and they are hardly ever hospitalized. Not one Virginian under the age of 20 has died from the virus.
The odds of contracting a case serious enough to be hospitalized increase with age. Very few people under 30 are hospitalized, but after 30, the odds don’t vary dramatically between age groups. Deaths are rare among Virginians under 50, and not likely for anyone under 60. But patients over 80 are extremely vulnerable, accounting for more than half of all COVID-19 deaths in the state.
None of this is especially revelatory. The data shown here tell us what we already know. But this presentation helps clarify thinking on some key public policy issues.
School reopening. Should Virginia schools re-open next fall? It depends upon whose perspective we take. From the perspective of K-12 students themselves, the risks are close to non-existent. A small number will contract the disease, but almost none will get sick enough to require hospitalization. Barring a fluke case, none will die.
From the perspective of teachers and parents, who fall into older age brackets, the perspective is different. Because so few young people get the disease, very few are carriers. Accordingly, the risk of contracting a disease from a school kid is far lower than, say, hanging out at a crowded bar or living in a nursing home. But that doesn’t mean the risks are trivial. Perhaps any back-to-school movement needs to be accompanied by strict enforcement of sanitary measures, such as frequent use of hand sanitizer, and/or the enforcement of social distancing for older teachers and staff.
Long-term care facilities. At the other end of the age spectrum, the numbers remind us we need to focus preventive efforts on the elderly age groups most likely to contract the disease, to be hospitalized for it, and to die from it. In particular, we should to pay attention to nursing homes and assisted care facilities where the elderly are likely to come into contact with a large number of people. Not only are they more likely to catch the virus in such settings, they are far more likely to die from it.
According to VDA data, 2,902 confirmed COVID-19 cases, or about 14% of all identified cases in Virginia, have occurred in long-term care facilities. Likewise, about 15% of all cases leading to death have come from long-term care facilities. The enclosed nature of these facilities and the difficulty in maintaining social distancing for a population that requires such intensive personal care puts nursing home populations at special risk. Unlike schools, we can’t shut them down. There is nowhere else for the residents to go. But stricter measures that would not be tolerated in other settings, along with more extensive testing and contact tracing, may continue to be advisable for nursing homes.
Workplaces. Virginia workplaces are dominated by the four age groups between 20 and 59, with a smattering of over-60 Virginians. Policies should be crafted for the unique demographics of those age groups. Given their demographics, the risk of contracting and spreading the disease is greater in workplaces than in schools, although a relatively small percentage of the working-age population will end up hospitalized, and a very small number will end up dying. Conditions will vary widely, however. Some businesses employ mostly young people, others employ more middle-aged people. Some businesses require close personal contact, others don’t. Some businesses can mix telework with in-office work, others cannot. A blanket, top-down policy decided by the Governor for the entire state does not make sense. Businesses should be trusted to do what’s best in their situation, and the state should step in when hot spots develop.

