

by James A. Bacon
The Northam administration has issued new guidelines urging unvaccinated students and staff to keep wearing masks in K-12 schools this fall — but won’t require them to do so. Some school districts, like Chesapeake, have voted to nix the masks, while others, like Virginia Beach (see Kerry Dougherty’s column below), will make the masks mandatory.
The Virginia Department of Health’s “Interim Guidance for COVID-19 Prevention in Virginia preK-12 Schools” says the mask mandate should remain in place until there has been sufficient time to allow for children under 12 to be fully vaccinated. The VDH follows the recommendations of the American Academy of Pediatrics. On the other hand, the Center for Disease Control has said vaccinated teachers and students need not wear masks.
Does a mask mandate for schools make sense? News accounts provide no data to help Virginians reach an intelligent judgment. Bacon’s Rebellion steps in to fill the void.
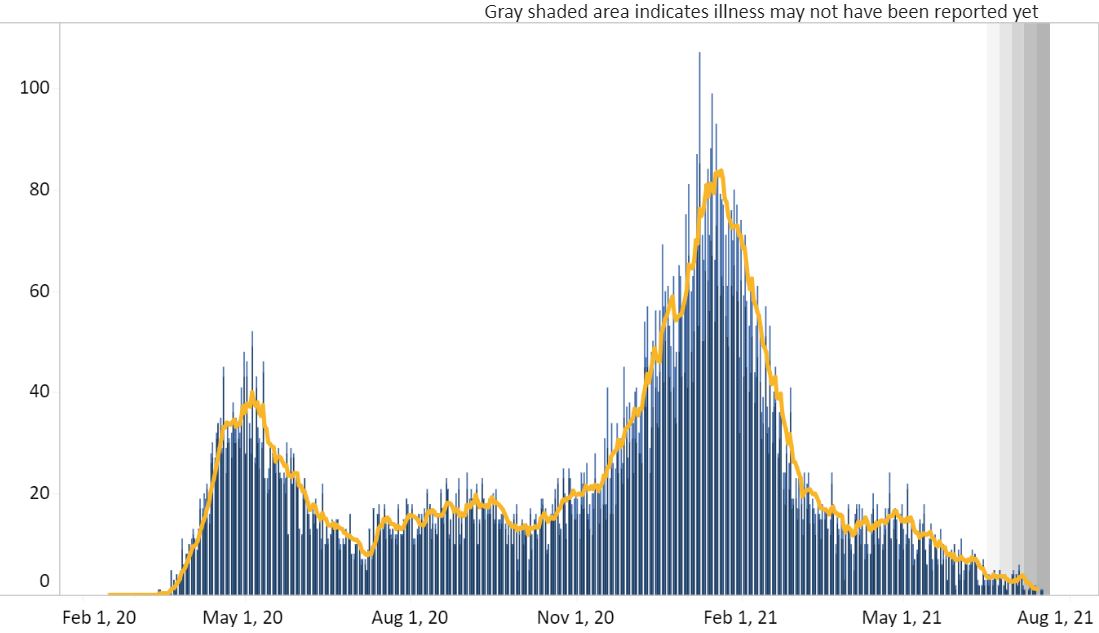
The big picture. The debate over masks in schools occurs against a backdrop of resurging COVID-19 cases as the highly transmissible Delta variant becomes the dominant strain. In line with national trends, Virginia has experienced a rise in cases. However, as seen in the graph above, the number remains far below the levels seen earlier in the year.
Meanwhile, the number of hospitalizations and deaths has barely budged (although it is important to note that the reported numbers of both could be understated due to delays in collecting and publishing data).

Virginia is in a very different position regarding the virus than it was a year ago. In a state of roughly 8.5 million people, there have been more than 10 million vaccination doses given. The VDH says 4,500,000 Virginians are fully vaccinated and another 500,000 have received at least one dose. Meanwhile, there have been 688,000 confirmed cases; COVID survivors enjoy a resistance to the virus comparable to that of people with vaccinations. Insofar as some COVID survivors have been vaccinated (providing even more robust protection), there is some overlap between the two groups. But a good estimate is that some 75% to 80% of Virginia’s population is inoculated against the virus. That explains the subdued spread of the hyper-virulent Delta variant.
Young people and the virus.
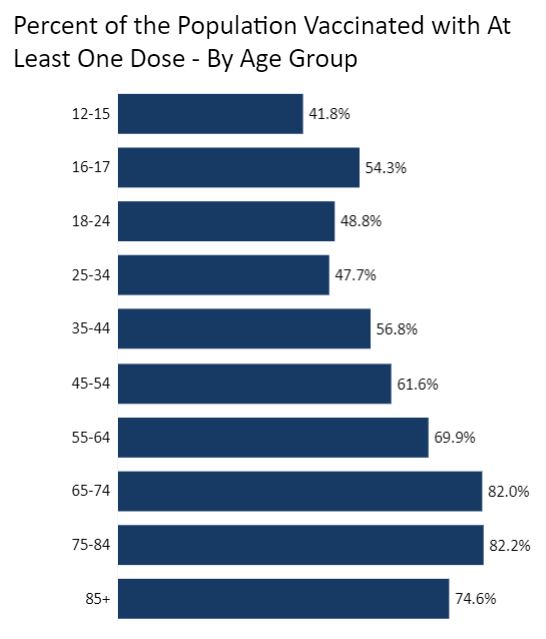
More than half (54%) of Virginians in the 16- to 17-year-old cohort have received at least one vaccination. The percentage for the 12- to 15-year-old cohort is 42%. In other words, nearly half of older school-age youths have resistance conferred by vaccination.
Those vaccinations provide protection over and above the fact that young people are far less vulnerable to COVID-19 in the first place.
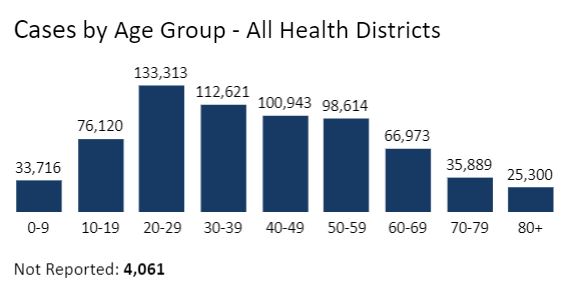
In the graph below we can see that young people (19 and under) account for fewer COVID cases than older groups, excepting the two elderly (70 and 0ver), age brackets, which are smaller age cohorts.
The chart below is where the story gets interesting. School-age children are far less likely to be hospitalized from the virus — only 630 instances reported throughout the entire epidemic.
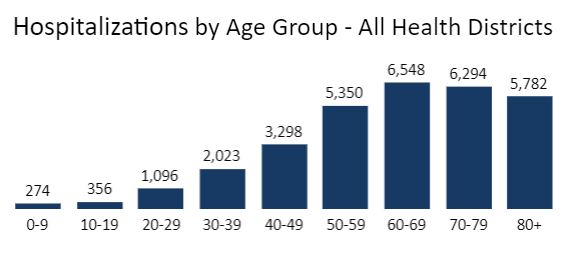
Now for the most pertinent data points of all… There have been only seven deaths among school-age children in Virginia over the course of the entire epidemic.
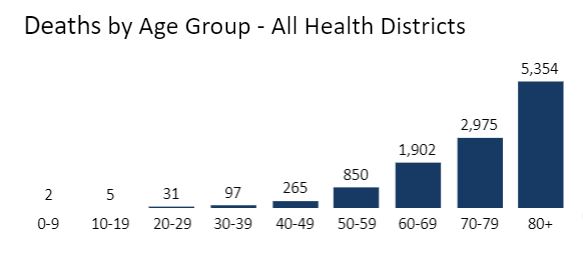
Of those seven deaths, VDH attributes only two to “outbreaks” occurring in K-12 settings, likely at one of the private and public schools that continued in-school learning through the height of the pandemic.
Summing up. Community spread of the COVID-19 virus is running about 6% of the peak, although that percentage could increase as the Delta variant gains momentum. Daily hospitalizations are running around 7.5% of the peak. And daily deaths are running at 1.2% of the peak. Against that backdrop, nearly half of 12- to 17-year-olds have been vaccinated, and every school teacher and staff person who wants a vaccination has had ample opportunity to get one. Any reduction in hospitalizations and deaths in the school-age population attributable to mandatory mask wearing could be too negligible to measure.
Conversely, the wearing of masks has non-trivial drawbacks. First, prolonged mask wearing results in increased inhalation of carbon dioxide, leading to hypercapnia or elevated CO2 levels in the blood. Hypercapnia is associated with irritability and dizziness. Second, prolonged mask wearing leads to breathing through the mouth instead of the nose, which reduces saliva levels in the mouth. Low saliva levels, dubbed “mask mouth,” contribute to bad breath, tooth decay and gum inflammation. These adverse effects have not been well studied, so the risks cannot be measured with any certainty. But the effects are well documented.
Are the benefits from mandatory mask wearing worth the risks? There is no evidence that the Northam administration has made a serious, independent effort to answer that question. If someone actually has, the evidence should be released to the public.
At least we can be grateful that Team Northam is allowing local school districts to make their own decisions.
{kind=link}
Leave a Reply
You must be logged in to post a comment.