

by James C. Sherlock
From the CDC:
Chronic diseases have significant health and economic costs in the United States. Preventing chronic diseases, or managing symptoms when prevention is not possible, can reduce these costs.
Virginia pays a great deal of money every year to contractors who manage the care of its Medicaid population.
It is a hard job, but even though the challenges are tough, it has appeared to me for a long time that we are not getting our money’s worth from $18 billion annually in Medicaid payments for the populations managed by these contractors.
A white paper, “Prevent Costly Chronic Disease Through Member Engagement” caught my eye as the basis for a follow up to my earlier report on public health and Medicaid managed care in Petersburg.
This is that update.
From that white paper:
The United States is experiencing a chronic disease crisis. Currently, 6 in 10 adults in the U.S. have a chronic disease, 4 in 10 have two or more chronic diseases and millions more are at risk of developing a chronic disease, according to the Centers for Disease Control and Prevention.
When plan participants develop a chronic condition, medical claims skyrocket. In fact, 85% or more of health insurance costs nationwide are related to chronic conditions.
With this in mind, health insurance companies are looking for ways to reduce their claims costs by keeping their members healthy. Unfortunately, when it comes to various prevention efforts — such as most diabetes prevention programs — too many members fail to complete the curriculum or achieve their goals.
The health care of virtually all of the Medicaid insured population of Virginia is under management by Department of Medical Assistance Services (DMAS) contractors.
The National Committee for Quality Assurance (NCQA) accredits managed Care organizations through a process of evaluating against a set number of measures of performance, quality, and outcomes. Those accreditations have not translated to good performance of those organizations in certain parts of Virginia.
The Medallion 4.0 program provides access to acute primary care services, prescription drugs and behavioral health services for most of the Medicaid population. To wit:
Populations covered by the Medallion 4.0 program include pregnant women, children, low income parents and caretaker relatives living with children, FAMIS members, and current and former foster care and adoption assistance children.
Some of the Medallion 4.0 priorities include engaging health systems and stakeholders, as well as providing holistic and integrated care to covered members.
The ability of Medicaid members to choose among contractors is meant to be the incentive for good performance. It certainly can be and in most environments is. But it is difficult to assess whether that choice, while well meant, is effective in practice for a poor and generally low-information Medicaid population.
The Commonwealth Coordinated Care Plus Program is Virginia’s program to manage mental health services for every Virginian needing them regardless of insurance coverage.
Individuals receiving services through CCC Plus do so in a nursing care facility, or through one of DMAS Home and Community Based Services 1915(c) Waivers. The CCC Plus program provides services and care to approximately 267,700 lives as of January 15, 2021.
Medicaid managed care programs are profitable lines of business with no patient outcome risk participation by contractors under current contract structures. From here I will refer to Medallion 4.0 specifically.
The Medallion 4.0 Managed Care Services agreement can be seen here. The referrals to section numbers hereafter refer to that contract.
Contractors are paid a percentage of the money they handle. (Section 6.1.D).
The Contractor shall be entitled to a capitation payment for the member based on the recoupment/reconciliation procedures in Section 15.8 and the Managed Care Technical Manual.
Each contractor is required to have a Quality Assessment and Performance Improvement Program (section 9.3).
Each is required to report on its Healthcare Effectiveness Data and Information Set (HEDIS) measures annually.
The Contractor will assure annual improvement in these Medicaid HEDIS measures until such time that the Contractor is performing at least at the 50th percentile for “HMOs” as reported by Quality Compass. Thereafter, the Contractor is to at least sustain performance at the Medicaid 50th percentile. The Contractor is encouraged to set goals to support the Department’s goal of attaining the seventy-fifth (75th) percentile for each of these measures. (Section 9.9)
Section 9.10 defines other measures of effectiveness including:
…clinical quality, access, and utilization measures using nationally recognized measure sets to track and trend MCO performance and to establish benchmarks for improving the health of Medicaid and CHIP populations served through the managed care delivery system.
The contract includes a performance withhold program (Section 9.18) and a Value-Based Payments (Section 9.19 feature
…to reinforce VBP principles by setting performance standards and expectations for Contractors in key areas influencing member health and health outcomes. By tying financial incentives to Contractor performance on designated quality measures, the PWP focuses performance attainment and improvement efforts on areas of high importance to members. This effort also aligns with the Virginia Medicaid focus areas by including measures pertaining to chronic conditions, prevention, and maternity care.
JLARC published a study “Managing Spending in Virginia’s Medicaid Program” that was critical of inefficiencies it found. The General Assembly mandated change. Section 9.20 responds:
To implement this mandate, the Department contracted with its actuary to identify clinical efficiencies (CE) under its managed care programs. The first set of CE analyses focus on medically unnecessary or potentially preventable spending for hospital admissions, hospital readmissions, and emergency department visits, as well as efficient utilization and management of prescription drugs.
Those were good things to do, but analysis of both Medicaid expenditures and public health shows they are not as important as chronic disease management.
All of that said, the performance incentives in the contracts are limited to a 0.25% withhold penalty on the capitation payments and a schedule of small fines before possible termination of the contract.
I have no idea how one-quarter of one percent capitation withhold was arrived at, but it seems very small. Then there is the list of Compliance Monitoring Process (CMP) fines.
The Department has a seven (7) level compliance point system within its CMP
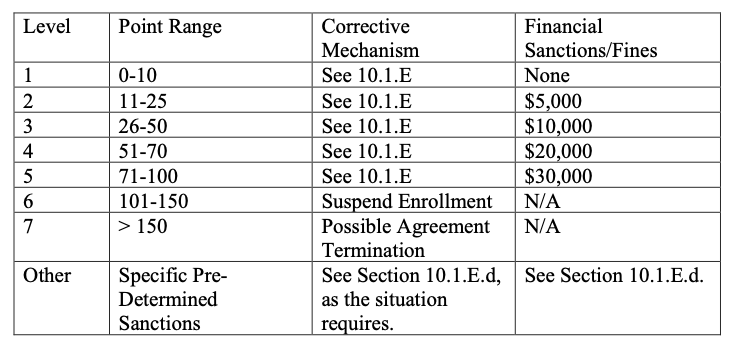
When one looks at how those points are accumulated, however, the one-point, five-point and 10-point violations descriptions (Section 10.1.E) make it appear that these fines are likely rarely if ever to prove financially significant even if DMAS detects them.
It would be useful to know how many penalties — capitation withholds, fines or dis-enrollments, have occurred in the history of the program. I will ask.
But given the very bad public health in Virginia cities and counties whose populations are dominated by persons insured by Medicaid, it is time to reassess:
- what is most important to the public health and how to achieve it through Medicaid;
- the contractor program;
- the design of current contracts;
- how they are managed by both DMAS and the contractors; and
- the incentive structure.
Leave a Reply
You must be logged in to post a comment.