
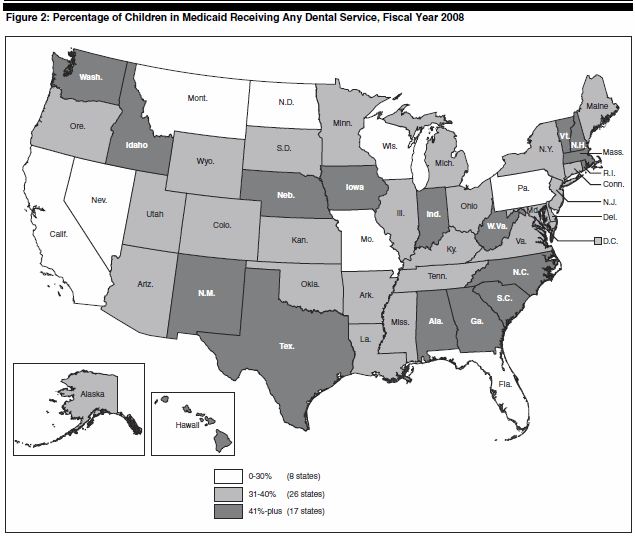
 Virginia falls in the middle tier of states for the percentage of children in Medicaid receiving dental service — somewhere between 31% and 40% — according to a recent study published by the Government Accountability Office. (Click on map for more legible image.)
Virginia falls in the middle tier of states for the percentage of children in Medicaid receiving dental service — somewhere between 31% and 40% — according to a recent study published by the Government Accountability Office. (Click on map for more legible image.)
The GAO estimated that 6.5 million children nationally had untreated tooth decay, and that rates of dental disease among children in Medicaid have not improved over time.
A big problem is the low participation rate of dentists in Medicaid and CHIP (the Child Health Insurance Program). Among those who do participate, many place limits on the number of Medicaid patients they will treat. Who would have figured? One solution would be to pay health care professionals enough so they don’t lose money for treating Medicaid patients. Of course, that would be expensive.
Another might be to expand the number of “mid-level” practitioners, or dental therapists, who can provide routine dental services like teeth cleaning and cavity filling, as they do in the U.K., Canada, Australia and New Zealand. But the use of dental therapists has been highly limited in the United States, according to the GAO: There is one program in Minnesota and another for Alaska Natives. In Minnesota, people can earn an M.A. degree in “dental therapy”, which is a much easier-to-surmount occupational barrier than earning a four-year Dental school degree.
Seven states (Virginia not among them) do allow dental hygienists and primary care physicians to provide certain dental services without the on-site supervision of a dentist. But these are limited mainly to preventive services.
The GAO report does not explicitly say so, but it appears that the American Dental Association (ADA) and its state counterparts keep a tight lid on who can practice dentistry and when — using their influence over state government licensing and higher educational programs to limit competition. Responding to the crying need to expand coverage, the ADA response has developed the position of “community health coordinator” to provide “oral health education” as well as limited preventive services. As of last summer, the program had enrolled 27 students in a pilot program. The ADA plans to train an additional 18 by September 2012. Woo hoo! That’ll really help close the gap for millions of poor kids!
What’s been going on in Virginia? I found this summary by the Children’s Dental Health Project.
In 1997, concerned about low utilization of dental services in Medicaid, the General Assembly ordered a study. The Department of Medical Assistive Services then convened a Dental Advisory Committee. Then in 2000, a coalition called Virginians for Improved Access to Dental Care formed. Legislative proposals were submitted in 2004. And actual programs were rolled out in 2006 — 10 years later.
The Virginia solution? The state Medicaid department contracted administration of the dental program through a vendor, Dora Dental, inc., which offered a number of administrative and billing improvements, and the state increased dental fees by 28%. An additional 190 dentists were credentialed to provide Medicaid and CHIP services. Children’s utilization of dental services increased from 29% to 36% by 2006.
That is still a pitiful number. I see no reason why dental hygienists or dental therapists should be banned from working independently to clean teeth, take x-rays, fill cavities and provide other basic services that they already do routinely in dentists’ offices. Dentists predictably will trot out the old “quality of care” argument. In other words, it is preferable to let two-thirds of Virginia’s poor kids go without dental care of any kind than run the risk that a handful might receive improper care. Such would be the logic of a craft union, er, profession, determined to protect its turf.

