

by James C. Sherlock
Either the title of this article or “the facility failed” is stock language used in every summary of a citation for a nursing home’s violation of federal regulation. It is the truth, but not the whole truth.
Inspectors come to a nursing home in Virginia once every couple of years. The staff of each chain-owned nursing home is instructed on what to do and how to do it and is closely monitored year-round by the chain’s regional operations and nursing representatives.
So, a change in the language seems appropriate.
Perhaps write “the management and staff of chain xxx, and the staff of the facility failed …” for each citation. That is the full truth and would enable both the Centers for Medicare & Medicaid Services (CMS) and state oversight authorities to track chain performance through a new metric.
The author, with a high tolerance for boredom, reads journalist reports and academic and government studies on the effects of ownership structures on the quality of care in nursing homes. Many make a great deal out of small differences. He decided to examine that topic in Virginia.
The differences here are stunning in their scale and consistency.
Consider some of the facts.
Ownership Structures
Virginia has 289 nursing home operating companies certified for Medicare and Medicaid, for Medicare alone or Medicaid alone. Of those, an assessment of ownership records reveals:
- 171 facilities owned by private equity;
- 60 by 501(c)(3)s;
- 23 by corporations;
- 14 by individuals;
- 12 by partnerships; and
- 9 by state or local governments.
CMS provides a Survey Summary database as a baseline to assess compliance with federal nursing home regulations. To that is added for this discussion:
- the names of the chains. Chains control all of the private equity facilities.
- The current staffing ratings and occupancy rates offer context for chain business models.
The chart below shows the chains with the highest average number of health violations per facility in the current inspection cycle.
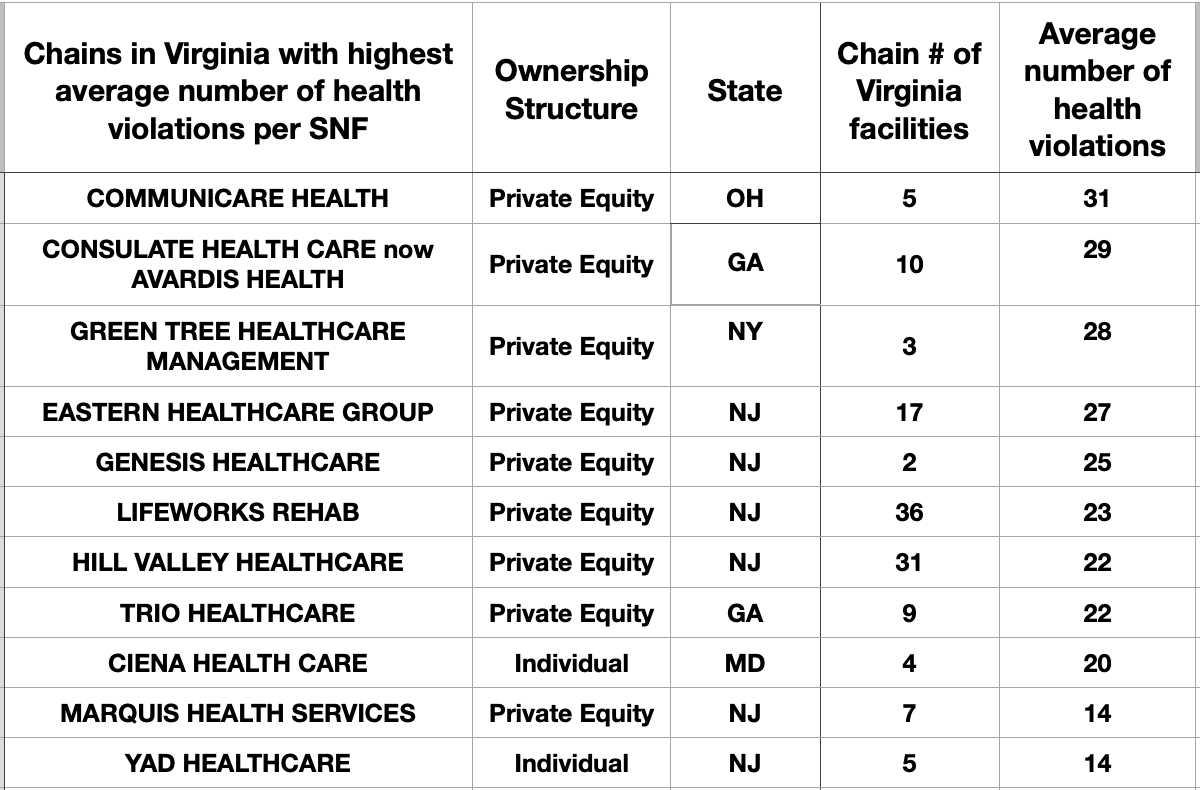
The picture gains focus in the curated spreadsheet (updated 14 Feb 9:38 AM), enhanced with additional contextual information and color-coded background fills. The color standard is red (worst), tan (poor), white (average), light green (good), and dark green (best). At a glance, it reveals a great deal of good and much bad.
Overall, the differences are incredibly dramatic. Those ten out-of-state chains operating in Virginia are the problem with low-quality nursing homes here, not part of it.
For context, let us examine the numbers beyond average health deficiencies. Those ten chains with the highest average health citations operate 129 facilities in the Commonwealth, accounting for 45% of Virginia’s total of 289.
Compared to the 56% of competent facilities, they boast:
- Six of six special focus status facilities in Virginia,
- 16 of 22 facilities with an abuse icon,
- 11 of 14 Immediate Jeopardy citations written by VDH inspectors,
- An average staffing rating of 1.54 out of 5. The rest of the state’s portfolio averaged 3.22 out of 5. The national average across 14,713 facilities for this metric was 2.89 out of 5 in the same month. Perhaps industry lobbyists will qualify their statement to the General Assembly next time about how impossible it is to staff nursing homes in Virginia. It is demonstrably hard for some, but not others, located mere blocks away.
- Average occupancy of 89%. How exactly does that happen? So much for Medicare Compare. The rest average 85%.
On average, the ten chains produce, compared to their competitors:
- Four times the average number of abuse, neglect, and exploitation citations,
- More than twice as many quality-of-life and care deficiencies,
- Twice as many resident assessment and care planning citations,
- More than five times as many nursing and physician services deficiencies,
- Three times as many violations of resident rights,
- Three times as many citations for nutrition and dietary deficiencies,
- More than twice the number of pharmacy services citations,
- Four times the number of environmental deficiencies, and
- Nearly five times as many administration deficiencies.
Heard enough?
Enforcement
CMS has long sought sufficient information on chains to develop oversight regulations. Chains continually deny CMS that information without consequence. The same thing occurs in Virginia licensing, with the same lack of sanctions.
Title 42 Chapter IV Subchapter G Part 488 Subpart F – Enforcement of Compliance for Long-Term Care Facilities with Deficiencies currently addresses only individual facilities.
A suggestion for CMS to cut the Gordian knot: add Chain Name and Chain Number to the inspection form header. Track the performance of chains in health surveys and complaint investigations. Then write a regulation requiring that chains meet minimum criteria for both average staffing and average inspection performance measured by citations and their severity over a cycle. Warning after one cycle, termination after two.
Bottom Line
The Health Commissioner has sufficient current licensing authority to prohibit nursing home chains and chain managers from operating in Virginia by making their absence a condition of facility licensure. § 32.1-19 Duties prescribed by Board:
C. The Commissioner shall ensure, in the licensure of health care facilities, that quality of care, patient safety, and patient privacy are the overriding goals of such licensure and related enforcement efforts.
The Virginia Department of Health can generate actionable information, similar to that demonstrated here. The next level of detail, the citations and their scope and severity, is provided in a second curated spreadsheet, also from CMS data.

There is a third level that provides access to the nightmarish details of the worst offenses.
Owners will sell under threat of loss of license to operate in this state, because that will trigger CMS to ban them from the Medicare and Medicaid programs altogether.
The author cannot see a downside.
Leave a Reply
You must be logged in to post a comment.