
by James A. Bacon

Aubrey Layne was a great public servant in Richmond before he moved back to Norfolk to take a job as chief administrative officer of Sentara Health. He did a superior job as Secretary of Transportation under Gov. Terry McAuliffe and then as Secretary of Finance under Gov. Ralph Northam. He earned my respect as a nonpartisan straight shooter. So, when he says that the Medicaid cuts enacted in the “Big Beautiful Bill” are a cause for concern, I pay attention.
In a recent Richmond Times-Dispatch column, he warns that Virginia “will face difficult decisions that could directly affect access to care for low-income families, children, seniors and individuals with disabilities.” Safety-net hospitals and rural providers who rely disproportionately on Medicaid revenues, he says, will be particularly hard hit.
In contrast to the hysterical, people-will-die narrative dominating Virginia’s news coverage, Layne argues that Virginia can handle the fallout of the Big Beautiful Bill — its various provisions will cost Virginia $26 billion over 14 years, according to the Virginia Department of Medical Assistance Services — through fiscally smart investments in primary care and the social determinants of health.
I wish he’d delved deeper in his analysis. What kind of investments in primary care? Which social determinants of health are even fixable? Indeed, is the magnitude of the problem remotely as bad as the sky-is-falling chicken littles are proclaiming? Admittedly, that’s a lot to ask of a 750-word op ed.
The Medicaid controversy is obscured by smoke and fog. Democratic politicians are manning the smoke machines and legacy media are running the fog generators.
It’s not clear how the pain of those $26 billion in cuts will be distributed between the Commonwealth, hospitals, and Medicaid recipients. Status-quo media has failed spectacularly to report all sides of the story. I haven’t seen a single article defending the cuts, and I couldn’t find one in the top four or five pages of Google search results.
In June Virginia Democrats estimated that 166,000 Virginians could lose their Medicaid coverage (and another 137,000 could lose their Affordable Care Act subsidies) based on the House version of the Big Beautiful Bill. So reported the Richmond Times-Dispatch a week ago.
But there’s more to the story. A primary objective of the law is to focus Medicaid on helping the most vulnerable populations and rolling back enrollment of able-bodied adults. According to a bill summary provided by the Association of State and Territorial Health Officials (ASTHO), the law requires able-bodied adults aged 19 to 64 to work (or perform other qualifying activities) for at least 80 hours a month.
However, the law provides abundant exemptions — for pregnant women, people with serious medical conditions, tribal members, and parents of young children with a disability. Further, states can issue waivers for individuals facing short-term hardships such as natural disasters and high unemployment rates within their county.
Medicaid was set up to create a medical safety net for the indigent and elderly. It has expanded relentlessly, especially during the COVID pandemic. To what extent does the Big Beautiful Bill represent a retraction to benefit levels that preceded COVID? Politicians, pundits and news reports don’t say. Once an entitlement program expands, even if to cope with a temporary emergency like COVID, any regression toward the norm is attacked as a heinous cut in benefits to the vulnerable and needy.
Here, for your edification, are the top-line Medicaid enrollment numbers in Virginia for each July from 2019 through 2025 — data you won’t see anywhere but Bacon’s Rebellion because we’re the only media outlet interested in providing the context.
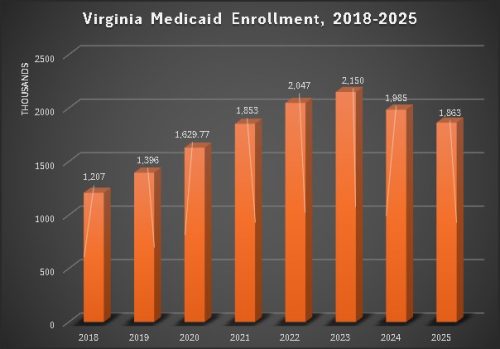
Virginia’s Medicaid expansion began contributing to enrollment growth in 2019, peaking at 750,000 additional enrollees over the base program in May 2023, and sliding back to 613,000 in July 2025.
The hypothesized loss of 166,000 enrollees would bring the number of enrollees down to about 1,700,000 — still higher than before the COVID epidemic that inspired “temporary” Medicaid expansion measures to assist people who lost their jobs from the shutdowns. Has that factoid been reported even once in Virginia media? If so, I haven’t seen it.
An ancillary issue is the impact on rural hospitals. News reports are warning that shrinking Medicaid enrollments will represent a fiscal calamity for financially marginal hospitals in center cities and rural areas. Maybe it will, maybe it won’t. Show us some numbers.
Most rural hospitals in Virginia belong to large nonprofit health-care systems. (There are very few if any independent hospitals left.) So, whose ox is getting gored? Small community hospitals or the big monopolistic health systems of which they are part?
No health system, I might remind Layne, is bigger and more monopolistic than Sentara. The Virginia Health Information Foundation website reports profitability for its individual hospitals, but hospital P&Ls don’t help an outsider understand the profitability of a health conglomerate that includes physician practices, health insurance companies, diagnostic centers and outpatient surgery centers. For all the public knows, hospitals function as loss leaders that funnel business to the most profitable units of the enterprise.
In his op ed, Layne notes that in 2014 Sentara provided $174 million in uncompensated care and $40 million to nonprofits addressing social determinants of health. Interestingly, Sentara Health does not publish an annual report that provides system-wide profits, much less a breakdown of revenue and profit by business line, so we can’t evaluate the significance of those numbers.
The other big question is this: What happens to the anticipated 166,000 Virginians expected to be cut from the Medicaid rolls? How many will end up enrolling in the Affordable Care Act’s subsidized medical insurance marketplace? How much of lost Medicaid revenue will be recouped through Obamacare? Any estimate of the Big Beautiful Bill’s fiscal impact on Virginia that does not address that question is more worthless than a used hypodermic needle.
It’s conceivable that those who decry the Big Beautiful Bill will prove to be right. At this point, I’m not saying they’re wrong. But I’m not going to take the warnings of impending disaster on the word of Democratic politicians and legacy media. On the word of Aubrey Layne maybe. But only after he’s performed the in-depth analysis he did as a public servant.
Leave a Reply
You must be logged in to post a comment.