

by James C. Sherlock
Evidence of intentional wrongdoing by specific nursing home chains operating in Virginia is hiding in plain sight. The huge gaps and consistent trends in each exhibit below cannot be attributed to happenstance. It reflects business models rigorously applied.
The numbered exhibits draw entirely on a single Center for Medicare & Medicaid Services (CMS) file, Provider Information.
Medicare Compare rankings, patient acuity and occupancy
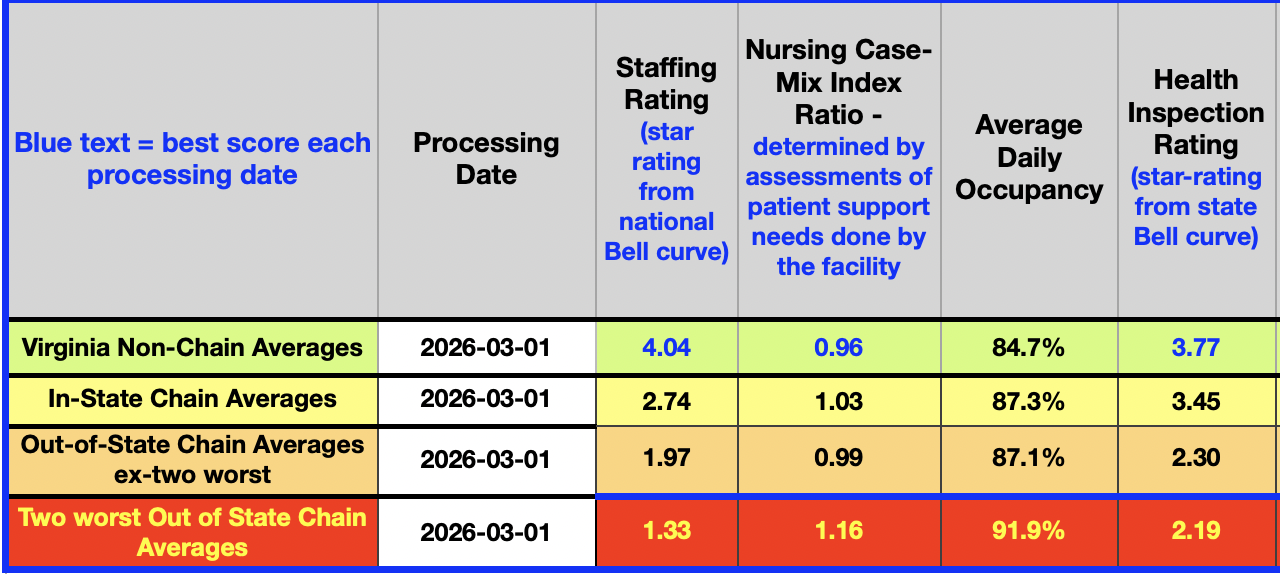
Exhibit One:
- Progressively lower-staffed facilities have residents with progressively higher average needs (nursing case-mix-index (CMI) ratio) for medical and activities-of-daily-living support. The national average CMI is 0.99; the two worst chains’ facilities have a CMI of 1.17, 18% higher. CMI ratios are directly proportional to Medicare and Medicaid reimbursements. They are derived from self-reported resident assessment results. That combination in evidence is unquestionably dangerous and amazingly profitable.
- Those facilities with the worst staffing and health inspection results have the highest occupancy. Hospitals can refer to Medicare Compare as easily as anyone else. It should influence hospitals’ selection of skilled nursing facilities with which they contract to transfer discharged patients who still need skilled nursing. A good regulator would review those contracts.
Nursing staffing
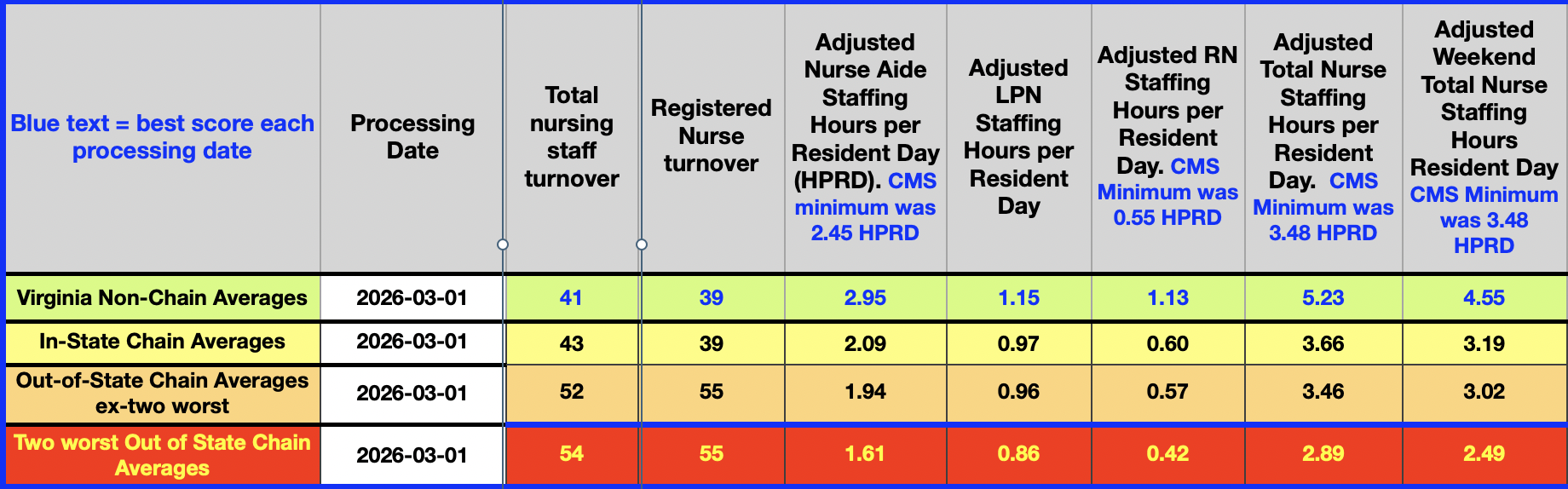
Exhibit Two:
The nurse staffing details follow the same trend as the staffing rankings. For comparison, the author has annotated the minimum standards developed by CMS. In Virginia, non-chain facilities easily surpass those standards. In general, out-of-state chains operating here do not. The worst chains are dangerously understaffed.
Health deficiencies
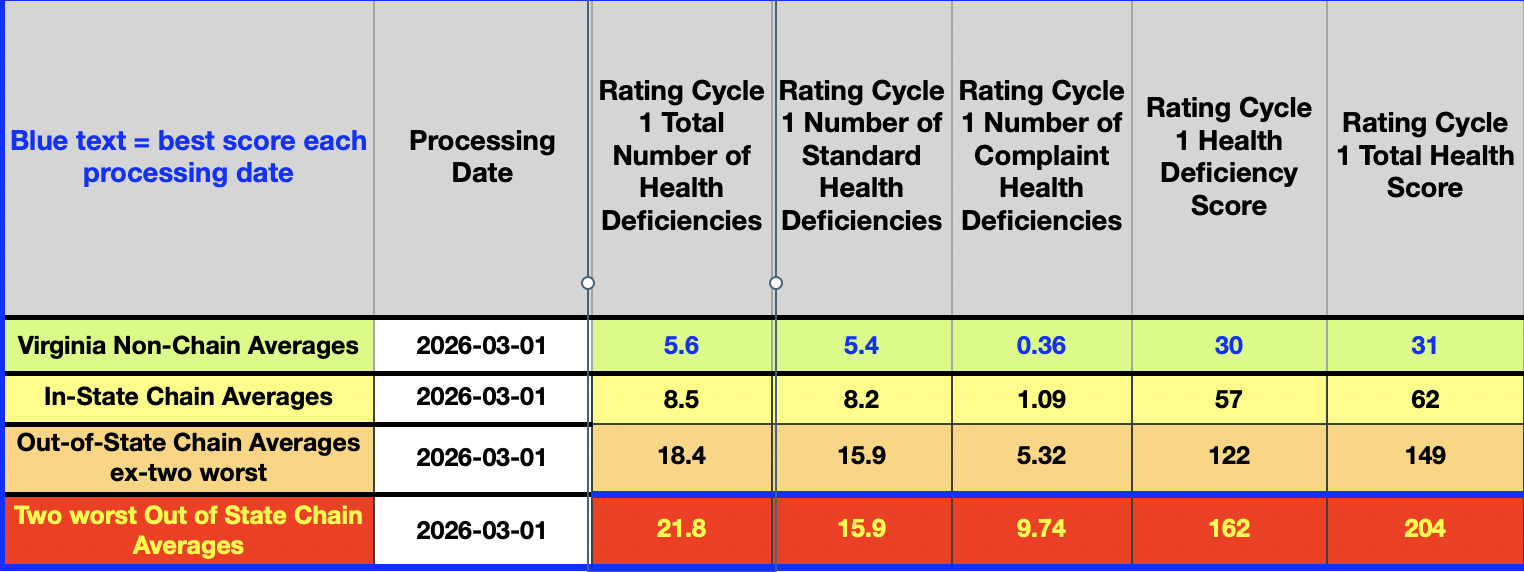
Exhibit Three:
Health deficiencies are reported by VDH inspectors conducting federal health surveys and complaint inspections under a VDH contract with the federal Centers for Medicare & Medicaid Services (CMS). “Deficiencies” is shorthand for the violations of federal law and regulations that are linked to each citation. The number of violations and their severity (scores) are reflected in the data. Again, huge and consistent gaps.
Sanctions
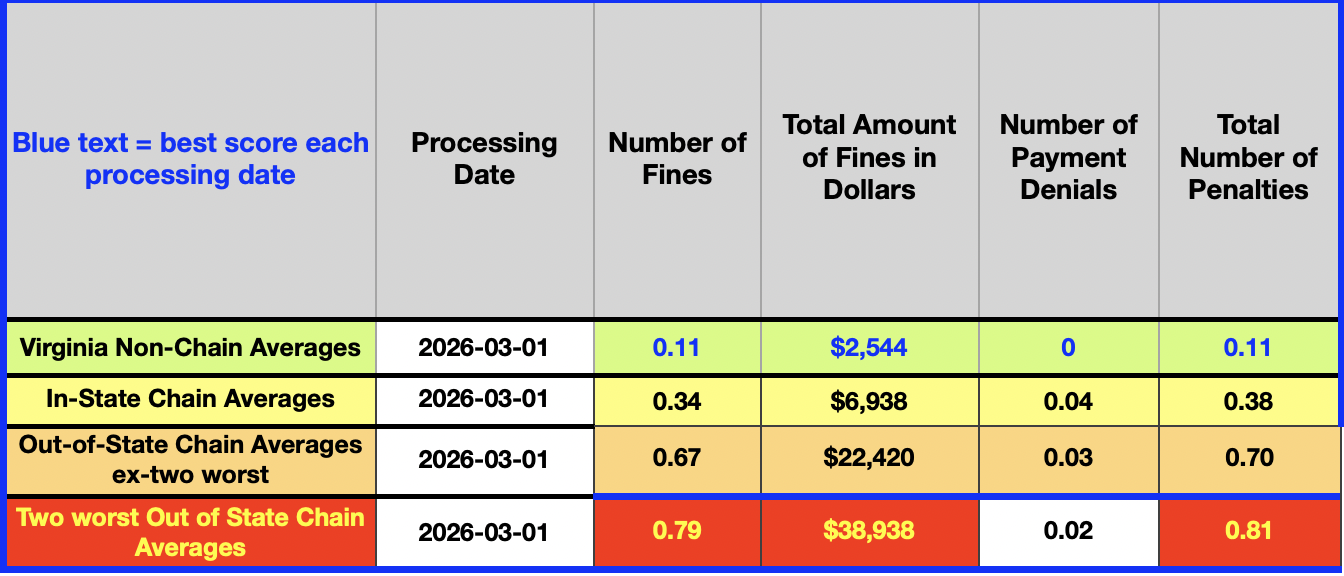
Exhibit Four
Sanctions are not proportional to the data in the first three exhibits.
Fines and payment denials displayed cover a three-year period. The $39,000 average fine for facilities in the two worst chains is less than half the cost of one RN in one year.
Temporary Medicare payment denials for new patients will typically be more expensive than the fines. Readers will note that payment denials are inversely proportional to the other data in the four exhibits.
The worst chains operating in Virginia
The two statistically worst chains operating here are Medical Facilities of America (MFA), dba Lifeworks Rehab, and Marquis Health Services (MHS). Please see an author-curated CMS data spreadsheet of Virginia facilities for confirmation.
Marquis, despite its track record, was permitted by the state to purchase seven more facilities in September of 2025. The headquarters of the two chains are four miles apart in Lakewood and Brick, New Jersey.
Property records show that both chains’ business models featured co-ownership of:
- an operating company LLC, which is the tenant and is paid by Medicare and Medicaid, and
- a realty company LLC, which owns the land and improvements and charges rent to the operating company.
MFA has sold some of its property companies to REITs to raise cash, but the proceeds have apparently not been used to improve staffing and performance at its facilities.
Virginia issues
Split oversight. The Virginia Department of Health (VDH) and the Department of Medical Assistance Services (DMAS) both have nursing home regulatory jurisdiction. So does the Virginia Department for Aging and Rehabilitative Services (DARS) Adult Protective Services (APS). The Attorney General investigates Medicaid fraud.
That split in responsibilities is a big part of the oversight problem.
State Licensing. The VDH nursing home license application gathers data
- neither on chains
- nor on the owners of the property that the operator leases.
Take, for example, the Virginia license application filed by MFA for its Chesapeake Health and Rehabilitation Center (Chesapeake). As annotated on that application by this author, the ownership information on that application differs from Chesapeake’s CMS SNF All Owners data, also provided by MFA, in every key respect.
The Virginia application does not inquire about the property owner. Property records for the location of Chesapeake show:
Both the redesign of the Virginia application and the reconciliation of the federal and state records seem appropriate. Give everyone a Mulligan with a new form that asks for:
- the same ownership information that they provide to CMS and
- the property ownership information they provide to local governments.
No extra work will be involved, and state records will finally be meaningful.
The General Assembly. The pronounced and consistent regressions of the magnitudes in the staffing and performance data above reflect business models rather than happenstance. They are demonstrably deliberate.
Yet the government of the Commonwealth acts as if chains and their business models do not exist. Virginia’s laws and regulations do not contain the word “chain” in relation to nursing homes. Not once in hundreds of pages of the Code of Virginia and the Virginia Administrative Code.
This author has tried and failed for years to break the official silence on the dangers the worst chains pose to frail and medically compromised Virginians.
Yet a few out-of-state chains in Virginia have been, and continue to be, in violation of every credible minimum health and safety standard in that industry. Indeed, Virginia’s own legislative efforts at setting staffing standards have been kept unacceptably low to accommodate them. For years, they have trailed by very large margins in nearly everything worth measuring except sanctions.
The core problem. Campaign donations are at the root of the problem and have been for decades. The industry buys influence like a farmer buys fertilizer, and for the same reason. It makes good things happen for the farmer.
In the most recent iteration, Governor Spanberger, Attorney General Jones, key General Assembly members, and their caucuses have taken large sums from the owners of New Jersey chains that joined together in 2025 as a new donor, Organizing for Virginia Seniors. To the credit of the House Republican caucus, they were skipped when the checks were issued.
The name is a bad joke. But bribery of public officials with unlimited donations is legal in Virginia. No limits. They are bought very cheaply considering what the payors get in return.
- Information on chains is not even sought.
- Chain business models are never mentioned.
- Virginia laws and regulations are silent on both matters.
- Fully-reported violations of federal law, including neglect and abuse of residents, are directly caused by the enforcement of chain business models.
- Sanctions are levied on facilities, not chains.
- The sanctions are easily absorbed by the enormous profitability of the worst chains’ models.
Bottom line
The author, having fought this fight for a decade, regrettably sees no reason to think that things will change meaningfully in Virginia. With the exception of updating the license application form, VDH cannot move aggressively without action by the General Assembly. If the past is prologue, the evidence presented here will roll off that particular duck. With honorable exceptions, the health and safety of nursing home residents and even the Colonial Heights scandal have not seemed to matter to a majority of our chosen representatives nearly as much as their own reelections.
Federal action is necessary, and far more likely. Unlike Virginia, CMS is actively trying to get a handle on chain performance. Here’s hoping the Justice Department is on deck.
Leave a Reply
You must be logged in to post a comment.