
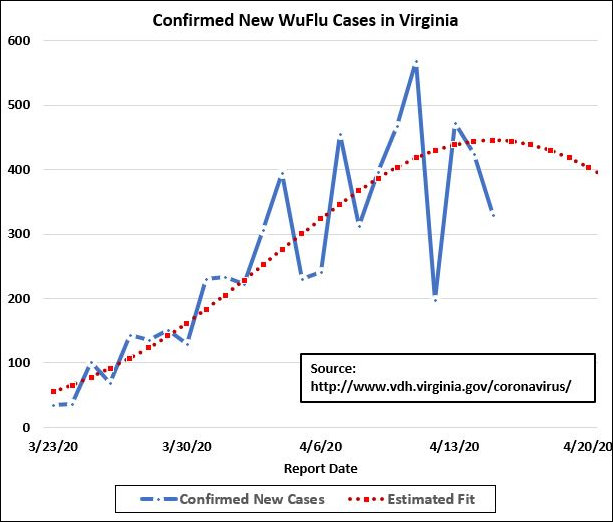
Sure looks to me like the curve is bending in Virginia, just as it appears to be around the world. The latest data from the Virginia Department of Health indicates 329 new confirmed cases of COVID-19 yesterday, less than the number eleven days ago. That’s consistent with what the Johns Hopkins University data is showing for the U.S. as a whole and for many other countries around the world.
The chart above, contributed by John Butcher, suggests that the spread of the virus in Virginia is peaking — assuming, of course, that current social-distancing controls stay in place. If we relax the measures, we can expect the epidemic to regain momentum. But the news is encouraging enough that Virginia public health authorities need to begin thinking about how to dial back social-distancing mandates on the margin in order to ease the devastating toll on the economy and restrictions on individual freedoms.
Here is our daily data summary:
COVID-19 spread
Total tests: 44,168, up 1,406
Total confirmed cases: 6.500, up 329 from the previous day
% tests positive: 23.4% yesterday
Total hospitalizations: 1,048, up 70 from the previous day
Total deaths: 195, up 41
Total hospital discharges: 752, up 31
Hospital capacity
Available beds: 5,617, down 374
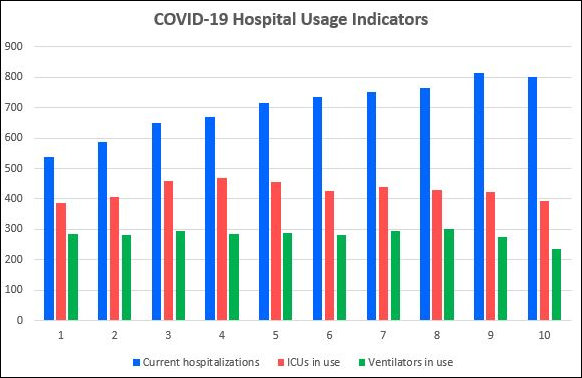
Currently hospitalized for COVID-19: 802, down 11
ICUs in use: 394, down 28
Ventilators in use: 234, down 42
While the incidence of new confirmed COVID-19 cases has flattened, that is only one measure. Because the measure is influenced by the number of tests taken — which, in determined is influenced by the availability of testing kits, it may not be an entirely reliable indicator. But several other indices are consistent with the idea that the epidemic is peaking: new hospitalizations, current COVID-19 patients in hospitals, ICUs in use, and ventilators in use. This data comes from the Virginia Hospital and Healthcare Association:
— JAB
Leave a Reply
You must be logged in to post a comment.