Hospital beds: Not enough
by James C. Sherlock
Virginians have read my complaints for years that Virginia’s Certificate of Public Need (COPN) law has artificially reduced supply of healthcare facilities in Virginia, driving up prices and reducing access. Legislators who believe as I do have not won the argument for the past 30 years in Richmond.
Unfortunately, I offer the tragic proof that the hospital industry can figure out how many hospitals, hospital beds and ICU beds are needed far better than bureaucrats can.
From Becker’s Hospital Review[1] 22 hours ago:
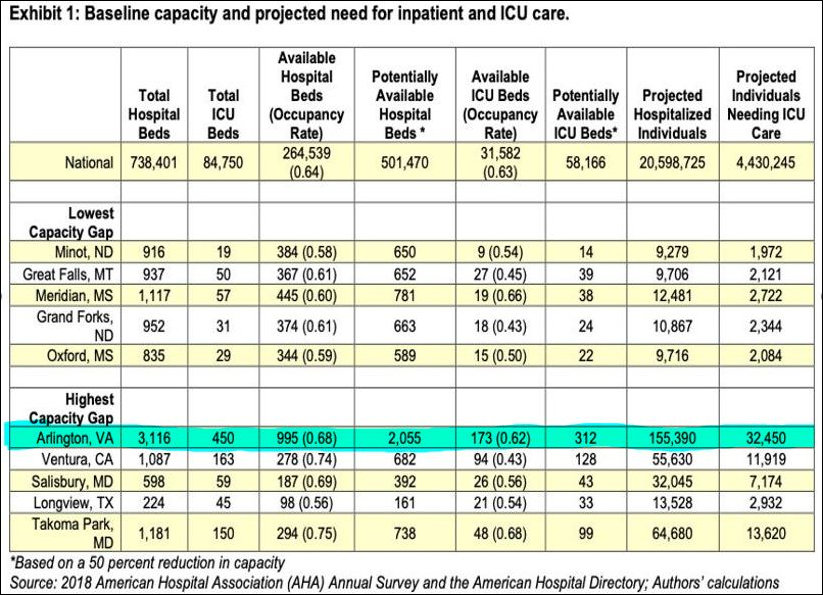
The demand for hospital beds in the U.S. is projected to far exceed capacity by mid-April, according to an analysis from the University of Washington’s Institute for Health Metrics and Evaluation in Seattle. … According to the model, 20 states will face a shortage of ICU beds when COVID-19 peaks.
Thirty five states and Washington, D.C., operated a Certificate of Public Need[2] program as of December 2019. Continue reading