
 by Carol J. Bova
by Carol J. Bova
A March 3 Virginia Department of Health (VDH) blog post discusses racial/ethnic “health and disease” disparities in light of the COVID-19 epidemic. It states that COVID case rates and hospitalization rates for blacks and Hispanics in the United States and Virginia are substantially higher than for whites.
“Social determinants of health are maldistributed,” concludes the blog post. “These disparities will continue health problem by health problem until there is more equity in the distribution of social determinants of health across racial/ethnic groups.”
Not so fast. There are two problems with this framing of the issue. First, the Northam administration’s obsessive focus on the color of peoples’ skin distracts from targeting the real factors influencing COVID mortality such as rates of obesity and diabetes. The second is that, ironically, VDH isn’t even doing a good job of measuring race. The assertions about differential case and hospitalization rates are based on deficient data.
As an example of the data issues Virginia is dealing with, the Virginia Hospital and Healthcare Association report of COVID hospitalizations shows 49,126 persons were discharged and 1,013 were still hospitalized as of March 14. The VDH hospitalization number of 25,323 is half that. because they count only those hospitalized when they first learn of a case If VDH is ignoring half of all hospitalizations, can any conclusions be drawn from the data?
Similarly, a Feb. 5 Centers for Disease Control (CDC) Morbidity and Mortality Weekly Report (MMWR), “Demographic Characteristics of Persons Vaccinated During the First Month of the COVID-19 Vaccination Program,” highlights problems with the statistics underpinning assumptions about racial disparities.
While data on sex was reported for 97% of recipients and age for 99.9%, the CDC article stated that data on race/ethnicity was available for only 51.9%. The range across jurisdictions administering vaccine doses was 0.2% to 100%. The large percentage of unknown race/ethnicity, says the CDC, means that “the findings presented in this study might not be generalizable to all persons initiating COVID-19 vaccination in the United States.”
VDH does concede some limitations to its data. In the fine print of a chart showing the Age-Adjusted COVID-19 Death Rates by Race/Ethnicity, VDH indicates that it uses the 2019 National Center for Health Statistics for “bridged” race and ethnicity, and the deaths per 100,000 are age adjusted to 2000 U.S. population standards.
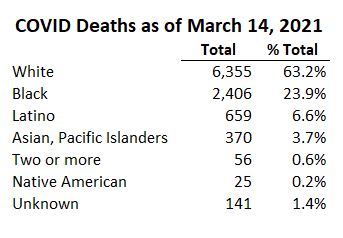 Then there’s the problem of unreported data. The VDH Death Rates chart goes through February 22, 2021, and on that day, VDH was still saying, “VDH is now processing 2021 death certificates related to the post-holiday surge of COVID-19 cases. As a result, a larger number of deaths is expected to be added by report date.” How many of the 2,402 deaths added to the total since then were prior to February 22?
Then there’s the problem of unreported data. The VDH Death Rates chart goes through February 22, 2021, and on that day, VDH was still saying, “VDH is now processing 2021 death certificates related to the post-holiday surge of COVID-19 cases. As a result, a larger number of deaths is expected to be added by report date.” How many of the 2,402 deaths added to the total since then were prior to February 22?
VDH also acknowledges “missing race and ethnicity data continues to be an issue. While death records are mostly complete, the case, hospitalization, and vaccination data reported above still reflect significant amounts of missing data. VDH has adopted an imputation method to fill these gaps. More information using this method will be available in the coming weeks.” (My emphasis.)
An article in the American Journal of Clinical Nutrition said: “The highest rates of obesity occur among population groups with the highest poverty rates and the least education.” Again, obesity and conditions associated with it such as diabetes and hypertension increase the risk of COVID-19 complications and death. The CDC notes that the risk factors can affect all adults, not only people of color.
Instead of working with flawed racial/ethnic demographics, VDH should target vaccine efforts to neighborhoods with high rates of poverty where COVID-19 risk conditions are most likely to be found — whatever their racial/ethnic composition. But don’t hold your breath. That approach might get vaccinations to people who need them most, but it won’t advance the Governor’s racial disparity agenda.

